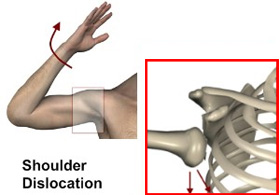
Shoulder Dislocation
Introduction:
lf your shoulder is wrenched upward and backward , you may dislocate it out of its socket. This condition is both painful and incapacitating. The force required is often that of a fall or a collision with another person or object.
 Etiology
Etiology
Most shoulder dislocation happen at the down front of the shoulder because of the particular anatomy of shoulder joint.
People with this injury appear in the ER in a fair amount of pain. Pain control is the first priority follows with X-Ray and if there are no bony injuries shoulder reduction is done.
Symptoms and signs
- Severe pain on shoulder joint
- Difficulty in moving the arm
Examination and Test Q
- Patient’s History
- Check for deltoid muscle (movement that causes pain)
- Pulse at the wrist, touch sensation
- X-rays–AP and Axial view of shoulder
Management
Closed Reduction
- The-Hippocratic method involves longitudinal traction on the arm and counterforce to the axilla , usually with the heel of the foot
- The kotcher method involves traction to the elbow with external rotation of the humerus and adducting the elbow toward the chest. This method is not currently recommended because of its association with neurovascular complications and proximal humerus fractures.
- Types of Analgesics
Some types of analgesic is combined with a sedative or muscle relaxant.
Shoulder dislocation in E/R
A 39 years old Nepali male came to emergency department at 2.00 am with complaint of Right shoulder pain (severe sudden onset) started when patient pushed heavy object continues rest relieving associated with deficalty in moving his arm 1 hour back.
On Examination: Patient looks ill, sweating in severe pain.
BP: 140/90, PR : 120/min.
Deltoid muscle is blatter actively
Radial pulse normal, normal touch sensation.
Classification: Anterior/Posterior/ Inferior.
Management: Right shoulder AP/Axial–shows that the humorous is separated from the scapula at the glenohumerous joint.
Treatment: Inj. Often 75 mg IM
Inj.Perfalgan 1 gm IV
Inj.Tramadol 50 mg lV
Reduction management using Hippocratic method.
Dr. Walid Abass Abdel Rahim
General Practitioner
GMCH& RC AJMAN
